
Neutrophils
Share
Follow Us
Neutrophilia is seen in any acute insult to the body, whether infectious or not. Marked neutrophilia (>25,000/µL) brings up the problem of hematologic malignancy (leukemia, myelofibrosis) versus reactive leukocytosis, including “leukemoid reactions.” Laboratory work-up of this problem may include expert review of the peripheral smear, leukocyte alkaline phosphatase, and cytogenetic analysis of peripheral blood or marrow granulocytes. Without cytogenetic analysis, bone marrrow aspiration and biopsy is of limited value and will not by itself establish the diagnosis of chronic myelocytic leukemia versus leukemoid reaction.
Smokers tend to have higher granulocyte counts than nonsmokers. The usual increment in total wbc count is 1000/µL for each pack per day smoked.
Repeated excess of “bands” in a differential count of a healthy patient should alert the physician to the possibility of Pelger-Huët anomaly, the diagnosis of which can be established by expert review of the peripheral smear. The manual band count is so poorly reproducible among observers that it is widely considered a worthless test. A more reproducible hematologic criterion for acute phase reaction is the presence in the smear of any younger forms of the neutrophilic line (metamyelocyte or younger).
Neutropenia may be paradoxically seen in certain infections, including typhoid fever, brucellosis, viral illnesses, rickettsioses, and malaria. Other causes include aplastic anemia, aleukemic acute leukemias, thyroid disorders, hypopitituitarism, cirrhosis, and Chediak-Higashi syndrome.
About Neutrophils:
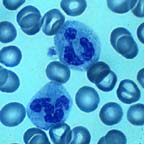
The most populous of the circulating white cells, they are also the most short lived in circulation. After production and release by the marrow, they only circulate for about eight hours before proceeding to the tissues (via diapedesis), where they live for about a week, if all goes well. They are produced as a response to acute body stress, whether from infection, infarction, trauma, emotional distress, or other noxious stimuli. When called to a site of injury, they phagocytose invaders and other undesirable substances and usually kill themselves in the act of doing in the bad guys.
Normally, the circulating neutrophil series consists only of band neutrophils and segmented neutrophils, the latter being the most mature type. In stress situations (i.e., the “acute phase reaction”), earlier forms (usually no earlier than myelocytes) can be seen in the blood. This picture is called a “left shift.” The band count has been used as an indicator of acute stress. In practice, band counts tend to be less than reliable due to tremendous interobserver variability, even among seasoned medical technologists, in discriminating bands from segs by microscopy. Other morphologic clues to acute stress may be more helpful: in the acute phase reaction, any of the neutrophil forms may develop deep blue cytoplasmic granules, vacuoles, and vague blue cytoplasmic inclusions called Döhle bodies, which consist of aggregates of ribosomes and endoplasmic reticulum. All of these features are easily seen (except possibly the Döhle bodies), even by neophytes.
The normal range for neutrophil (band + seg) count is 1160 – 8300 /µL for blacks, and 1700 – 8100 /µL for other groups. Keeping in mind the lower expected low-end value for blacks will save you much time (and patients much expense and pain) over the course of your career. Obesity and cigarette smoking are associated an increased neutrophil count. It is said that for each pack per day of cigarettes smoked, the granulocyte count may be expected to rise by 1000 /µL.


